Innovations in Behavioral Health
ED-based therapy with licensed social workers, a less-sedating medication strategy, and timely Tele-Psychiatry improves care and reduces avoidable admissions
The Challenge
Since the onset of the COVID-19 pandemic, there have been increases in Emergency Department (ED) visits for patients with Behavioral Health needs. The trouble is most EDs are not designed to treat Behavioral Health patients effectively. Traditionally, EDs conduct an initial evaluation, provide initial treatment, and medical clearance. When patients are amidst the most serious crises, EDs will often sedate patients for long periods or use physical restraints to stabilize them for psychiatric evaluation. This is the “sedate and wait” strategy. After stabilization, a common disposition is inpatient psychiatric hospitalization.
Yet with expanding nursing shortages, inpatient psychiatric beds are increasingly scarce, which results in prolonged ED boarding of patients with Behavioral Health needs, sometimes for days. This delays treatment for patients with Behavioral Health needs and can worsen their mental health as they wait for bed placement.
Currently, Behavioral Health patients rarely receive any talk therapy in the ED to try to de-escalate their crises. Furthermore, when Behavioral Health patients are waiting for inpatient bed placement, there may not be daily re-evaluations by ED Clinicians. These are important to assess whether the crisis has stabilized and patients can be discharged.
The Solution
USACS is the emerging market leader in innovative approaches to ED Behavioral Health. USACS has created and launched clinical management tools aimed at standardizing the upfront and ongoing care for Behavioral Health patients, and ensuring daily evaluation for possible discharge for patients boarding in the ED. One focus is reducing the use of sedating medications, such as haloperidol and lorazepam, in favor of medications that are less sedating, and target treatment of their underlying condition, such as olanzapine.
Another focus is a partnership with Array, the market leader in ED Tele-Psychiatry. In this model, ED patients with Behavioral Health emergencies are treated by a remote Array Psychiatrist rapidly after arrival with reassessments throughout their care to determine response to treatment. The intervention relies on providing early treatment to stabilize Behavioral Health crises. In addition, Array employs Behavioral Health counselors to integrate talk therapy into the ED, to start treatment and disposition planning at the beginning of care, rather than days later.
The goal of these strategies is to reduce time to treatment and to increase the ability to safely discharge patients to their home, rather than admit them, when admission can be avoided. Finally, USACS has developed a protocol for daily reassessment of ED Behavioral Health patients by ED Clinicians in observation status.
The Result
USACS has programs in Virginia and North Carolina with a plan to rapidly expand to other regions. Thus far, results have shown decreased time to evaluation, decreased inpatient admissions, and decreases in overall sedation. Furthermore, the opportunity to place patients in observation status if a prolonged ED length of stay increases the rate of re-evaluation, increases Clinician and hospital revenue, and often facilitates early discharge.
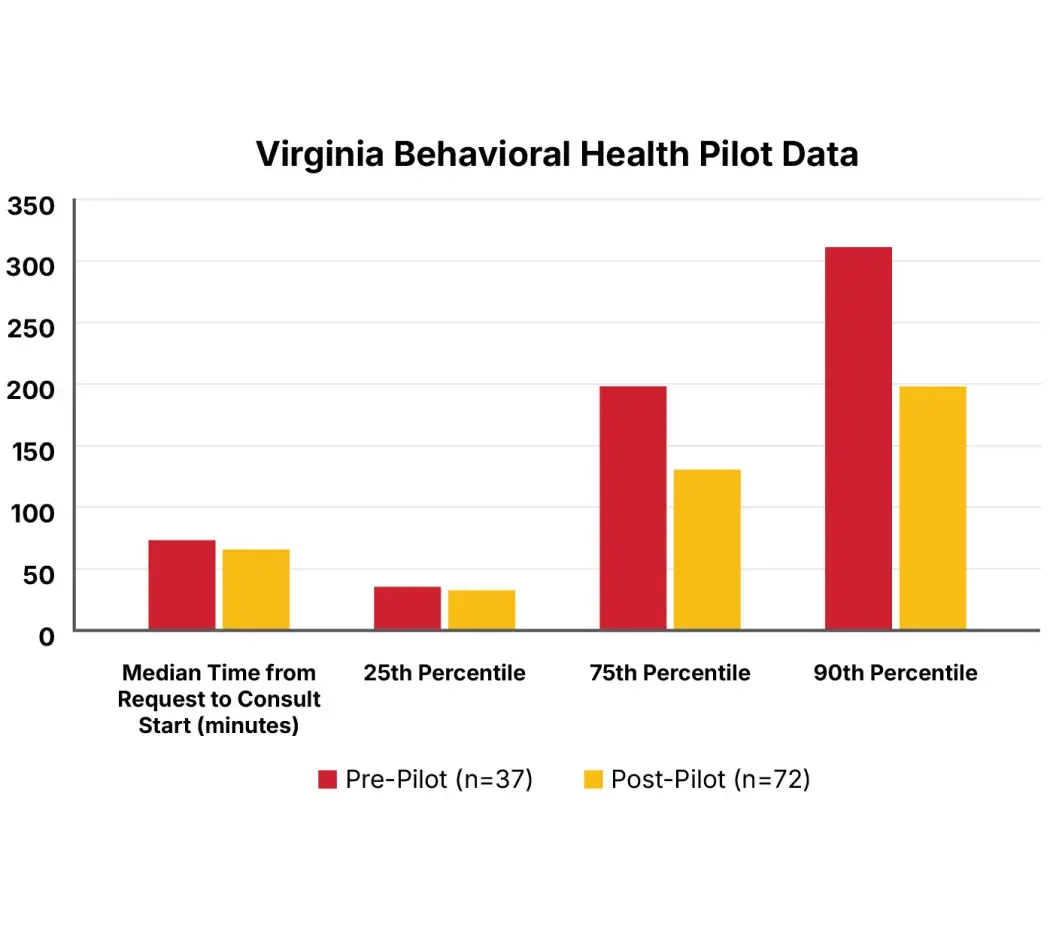
Early data from the Virginia pilot compared a two-month pre-period (n=37) to three-months of data post-pilot (n=72). The median time from psychiatric consult request to consult start decreased from 73 minutes to 65 minutes (a 11% reduction).
There were more dramatic effects for outliers, with the 75th percentile time to consult request to start time falling from 196 minutes to 129 minutes (a 34% reduction), and the 90th percentile falling from 307 minutes to 196 minutes (a 36% reduction). In addition, there was an increase in the ED discharge rate for Behavioral Health patients at mild risk from 50% to 80%.