Case Study: Leveraging the Dyad Partnership
| The Challenge
Nurse leaders and USACS medical directors unify teams to enhance care and drive improvements in throughput, quality, and patient experience.
Patients are best served when the nurses and clinicians who care for them respect and communicate well with each other and are united in the development and execution of the care plan. At US Acute Care Solutions (USACS), a physician-owned medical group that cares for more than 11 million patients a year, physicians and advanced practice providers (APPs) are trained and expected to work as a unified team with hospital staff. By investing in the dyad partnership between nurses and clinicians, many of USACS’ 400 acute care programs nationwide have seen exceptional results in quality, throughput, and patient experience.
“When physicians and nurses trust each other and are working hand-in-hand toward the same goals, we enjoy our days better, and we provide better care,” says Shaun Reynolds, MD, Medical Director of a Virginia Emergency Department (ED) that saw a 60% decrease in the percentage of patients who left without being seen (LWBS) after Reynolds and the ED Nursing Director implemented a dyad leadership strategy.
USACS’ executive nurse partners corroborate the medical group’s collaborative culture in client satisfaction surveys. Twice each year, USACS asks health system partners to complete a Net Promoter Score (NPS) survey sharing their likelihood to recommend the group to a friend or colleague on a scale of 0 to 10. Results are aggregated into an NPS, which can range from -100 to 100. Top brands score in the 50s or higher, including Amazon (58) and Costco (50). In its September 2025 survey, USACS earned an outstanding NPS of 76. Chief nursing officers rated USACS even higher, with a score of 78.
“USACS is a proven partner that helps us provide the high-quality care our patients deserve,” one CNO noted in his survey response. “They are considered an equal part of our team.”
The following examples show how USACS’ investment in the nurse-clinician partnership has helped partner hospitals in Virginia, California, and Ohio elevate patient care and clinical operations.
| The Solution
Driving Throughput Improvement in Virginia
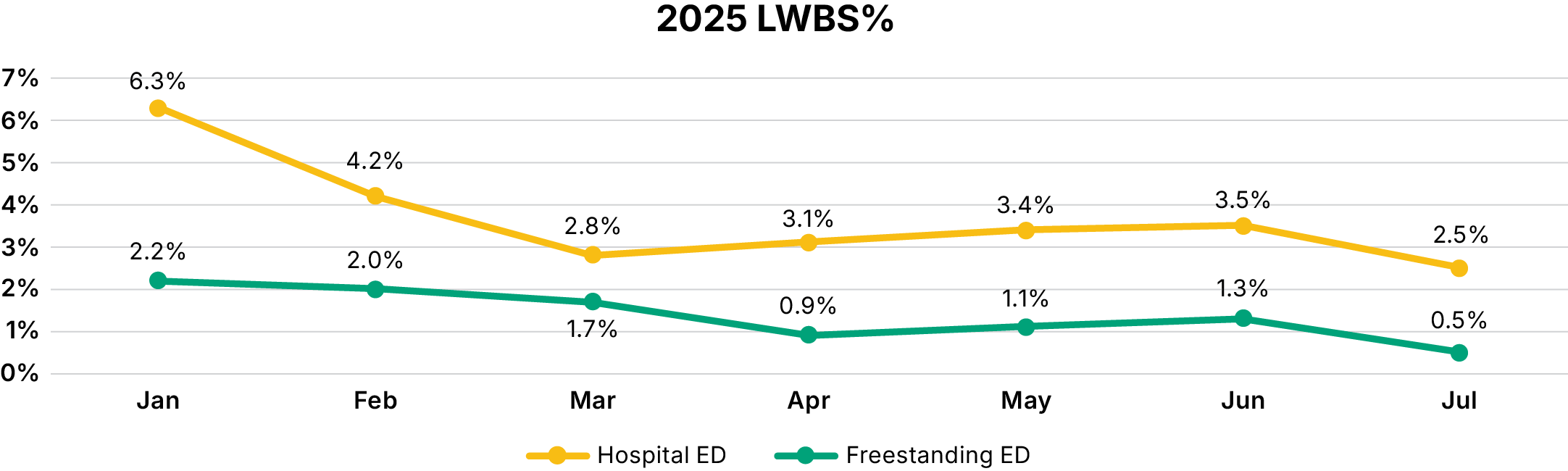
USACS partners with a nonprofit integrated healthcare system serving Virginia and North Carolina to deliver high-quality emergency medicine at six locations. These include a hospital in Hampton, Virginia, and a freestanding ED in nearby Newport News, which together see more than 100,000 patients annually. In the first half of 2025, USACS’ new emergency medicine Medical Director, Shaun Reynolds, MD, and the health system’s ED Director worked in lockstep to improve communication among nurses, physicians, and APPs. The EDs thrived under one unified team and in just six months, both achieved outstanding improvement in key metrics. At the main hospital, this included:
- 52% decrease in door-to-clinician time
- 17% decrease in discharge length of stay (LOS)
- 60% decrease in LWBS
- Patient experience consistently at or above goal
Strategies
Shared Goals & Expectations
Recognizing that their teams could only unite if they shared a single set of goals, Reynolds and the ED Director set out to clearly communicate that physicians, APPs, and nurses had collective responsibility for all ED key performance indicators (KPIs). To ensure that everyone on the ED team had the same understanding of the hospital’s expectations, the pair began posting performance goals on computers and in common spaces. Reynolds added KPIs and targets to orientation binders for new clinicians and articulated the expectation that they collaborate with nurses in striving toward these goals.
Dyad Leadership Rounds
Previously, Reynolds and the ED Director each conducted separate leader walks through the departments. Amid the busy 2025 flu season, they transitioned to dyad leadership rounds. Each Wednesday, they round through the EDs together, celebrating good performance, communicating with the team about new initiatives and priorities, and jumping in to grab a blanket or a glass of water for a patient. This has helped clinicians, nurses, and patients see them as a unified leadership team. It has also proven to be a far more effective communication tool than mass emails or text chains.
Open Communication
Leading by example, the two ED leaders are in constant communication and have empowered the nurses and clinicians in their EDs to approach each other directly to solve problems. Most charge nurses feel comfortable asking a clinician what might be holding up a patient’s discharge, and most clinicians will approach a nurse respectfully to inquire about delays in rooming patients. The open communication equips the team to quickly brainstorm together during volume surges and make temporary real-time adjustments to the flow model.
Celebrating Wins
When the EDs achieved three consecutive months in the green for patient experience, every member of the staff and each clinician received a small gift to recognize the team’s hard work and accomplishment. The shift to a collaborative ED culture has resulted in dramatic improvement in clinician and staff satisfaction.

“I’ve learned that when it comes to meeting patient flow and customer service goals, you really have to have partnership and collaboration and ownership between nursing and physicians. We really had to get on one page and have dialogue and camaraderie between the two.” -ED Director, USACS Partner Hospital
| The Results
Elevating Quality of Care in California
In January 2023, a large multi-state nonprofit health system expanded its partnership with USACS in California with the addition of the busy emergency medicine program at a Level II Trauma Center in Orange County. Under the previous medical group, the ED operated as a silo within the hospital and the relationship between clinicians and nurses was strained. Metrics lagged as a result. The hospital’s Director of Emergency Services & Trauma found an eager partner for change when USACS hired Jennifer Termeer, MD, as the new Medical Director of the ED in January 2024. Together they redefined ED culture and built trusting relationships with other hospital departments, proudly working to solidify the hospital’s position as the premier destination for acute care in the market. In the first 18 months of the partnership between Termeer and the Director of Emergency Services & Trauma, the ED experienced:
- 38% drop in door-to-clinician time
- 0.3% average LWBS rate
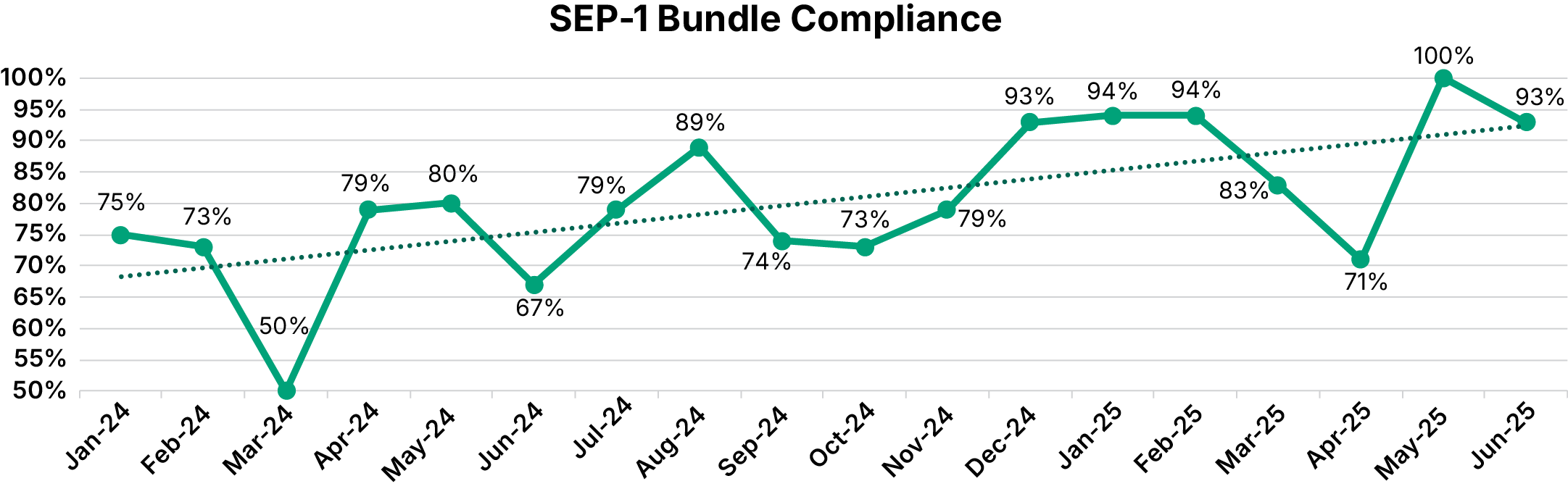
- 13% year-to-year increase in sepsis bundle compliance
- 75% drop in potentially redundant point-of-care testing
Strategies
Cultural Reset
Termeer and the Director of Emergency Services & Trauma aligned their leadership strategies and messaging to set the expectation that clinicians and nurses work together as a unified, transparent team. Physicians, APPs, and nurses all had seats at the table to identify opportunities for improvement in safety, quality, and efficiency. As examples, the leaders used their team’s feedback when
implementing new treatment-determines-placement guidelines, and when establishing a daily 12 p.m. nurse-clinician huddle to maximize the effectiveness of the ED’s vertical care model. With the improved working environment, ED nursing turnover dropped from 20% to 14% and several nurses who had left the department under the previous group returned.
Strong Hospital Relationships
The ED leaders rotated through other departments, meeting with the directors of surgery, obstetrics, and other specialties to hear their concerns about ED collaboration and identify opportunities to jointly improve patient care through stronger partnerships. One clear win was stroke care. Previously, the hospital’s neurologists received an average of eight consult requests from the ED per day for stroke patients, most for lower acuity cases that could have been diagnosed and managed in the ED. Neurologists helped Termeer and her nursing counterpart develop and train the ED team to use its own internal protocol for rapidly evaluating and managing patients who present with possible stroke symptoms. Average daily ED-requested stroke consults dropped to two, freeing up valuable time for the skilled neurologists who make the hospital a world-class stroke center.
Co-Investment in Quality
When USACS launched a sepsis treatment improvement plan in 2024 that included new early screening and alert processes to expedite decisions and orders, the Director of Emergency Services & Trauma partnered with Termeer to secure the team’s buy-in for the change. The hospital matched USACS’ investment, providing an additional nurse for the ED dedicated to monitoring clinicians’ adherence to sepsis and stroke best practices in real time. When the nurse identifies a potential fallout, the clinician is immediately prompted to consider ordering the sepsis bundle.
Resource Stewardship
The USACS team worked with the nursing staff in the last quarter of 2024 to eliminate automatic point-of-care testing during triage in order to avoid duplicate testing by clinicians. While nurses still conduct initial tests on appropriate patients, together the ED team achieved a 75% reduction in point-of-care testing. USACS also partnered with nursing to reduce redundant and non-emergent imaging in order to improve patient experience and ED throughput while saving costs. For example, the ED implemented a USACS evidence-based clinical management tool to help reduce MRI and CT imaging for atraumatic lower back pain, helping the hospital avoid unnecessary imaging in 87% of atraumatic lower back pain cases.
Enhancing Patient Experience in Ohio
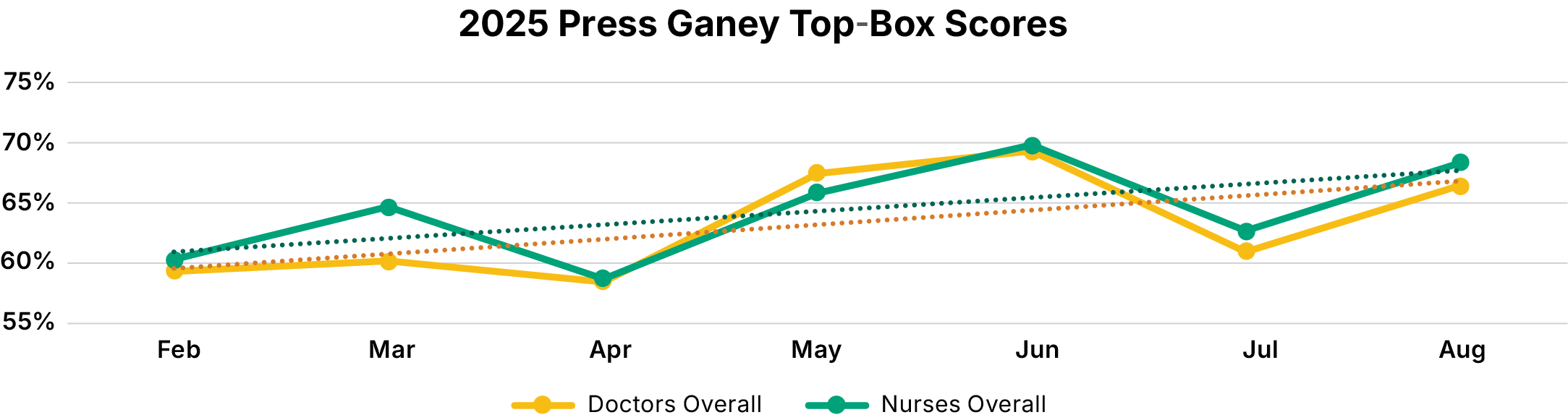
USACS, through its legacy companies, has partnered with a leading academic health system to provide quality emergency medicine services at a northeast Ohio medical center for more than a decade. USACS Medical Director Imran Tahir, MD, and the hospital’s ED Nurse Manager view the 43-bed ED’s clinicians and nurses as a single team with shared responsibility for the department’s goals. When patient experience scores dipped in April 2025, the two leaders collaboratively dissected the metrics to evaluate possible causes. With steady throughput, consistent ED volumes, and relatively low numbers of patients boarding in the ED, Tahir and the Nurse Manager launched an education campaign in staff meetings, team huddles, and one-on-one meetings to reinforce expectations for nurse-physician collaboration and jointly improve both clinician and nursing patient experience performance. Four months later, the ED had seen:
- 14% increase in Press Ganey top-box scores for the doctors’ overall domain
- 16% increase in the nurses’ overall domain
- 23% increase in the “staff worked together to care for you” domain
Strategies
United Teams
Whenever practical, a clinician or nurse entering a patient room asks the others to join. When a patient arrives by ambulance, nurses, technicians, and other members of the care team greet them and initiate care together. Clinicians are encouraged to take their time during patient exit interviews, ideally taking the nurse in the room with them.
Communication with Nurses
Patients with questions about their care should receive the same answer no matter who they ask. Physicians and APPs are expected to update nurses and any other members of a patient’s care team any time there is a change to the plan of care.
Team Language
When asked a question by a patient or colleague, clinicians and nurses should avoid using phrases like “I don’t know” and “that’s not my patient.” Instead, the ED team adopts a posture of “let me find out for you.” A patient or family member who appears lost
or confused is everyone’s responsibility. When a nurse or clinician encounters someone in the hallway, they should make contact, find the assigned nurse or clinician, and do a warm hand-off.
Best-Practice Patient Encounters
Nurses update whiteboards in patient rooms regularly to ensure patients remain aware of changes to their care team and plan of care. Physicians and APPs use best-practice behaviors when interacting with patients. These include sitting and making eye contact, establishing personal connections, and taking steps to ensure patients are comfortable, such as offering a blanket.
“Patients should see us as a team—medics, nurses, clinicians. We are all on the same team and we should all know the plan of care at all times.” -Imran Tahir, MD, Medical Director
About USACS
ln 2015, the nation’s premier acute care medicine practices formed USACS, a physician-owned and physician-led company that set forth a new model for acute care management. Every full-time USACS physician is offered equity in the company, accounting for 98% of ownership and empowering the group to recruit top-quality clinicians. The remaining 2% is held by health system partners, leaving USACS unencumbered by the volatility of private equity investment. Physician ownership aligns the missions of clinicians and hospital partners to drive better quality and value. Today USACS cares for more than 11 million patients annually across more than 400 programs in 27 states.