Reducing the Flow of Blood ... and Money
| The Challenge
Healthcare spending represents around 18 percent of the U.S. economy. By some estimates, 20 percent of that spending is squandered through various forms of waste. That translates to $600 to $850 billion each year. To put that in perspective, the 2009 stimulus bill, which was intended to rescue the entire US economy, cost $787 billion.
Many studies show that much of this waste actually results in poor patient outcomes, placing the true costs in human terms, as well as financial.
A huge proportion of wasted healthcare spending comes from over-utilization, e.g. unnecessary medical tests and treatment. Everyone has a responsibility to help fix such a gargantuan problem, from the patient who questions the need for that CT scan, to the government and private insurers who price reimbursements based on quantity of care provided. But Physicians groups and the individual doctors they employ are the ones truly on the front lines. And none more so than those who work in the Emergency Room.
We have sought to tackle the problem of over-utilization head on—but not just to do our part in containing financial costs. With many studies showing that unnecessary testing can result in worse patient outcomes, the focus on improving patient care demanded that we improve the way we order tests if we were to meet our responsibility to patients.
| The Solution
Where to Start?
As a culture, we look closely at our own behavior with a critical eye, seeking out clues to improve outcomes and reduce waste - which often are tied together. Analyzing our own data, we found huge discrepancies in the rates at which providers ordered blood cultures (Fig. 1). These tests are often ordered for patients who may have a sepsis diagnosis or to rule out a bacterial infection in the blood. But we found the usage rate of these tests was up to five times higher for some providers than for others. Seeing this as a potential area for improvement, we initiated a program of waste reduction.
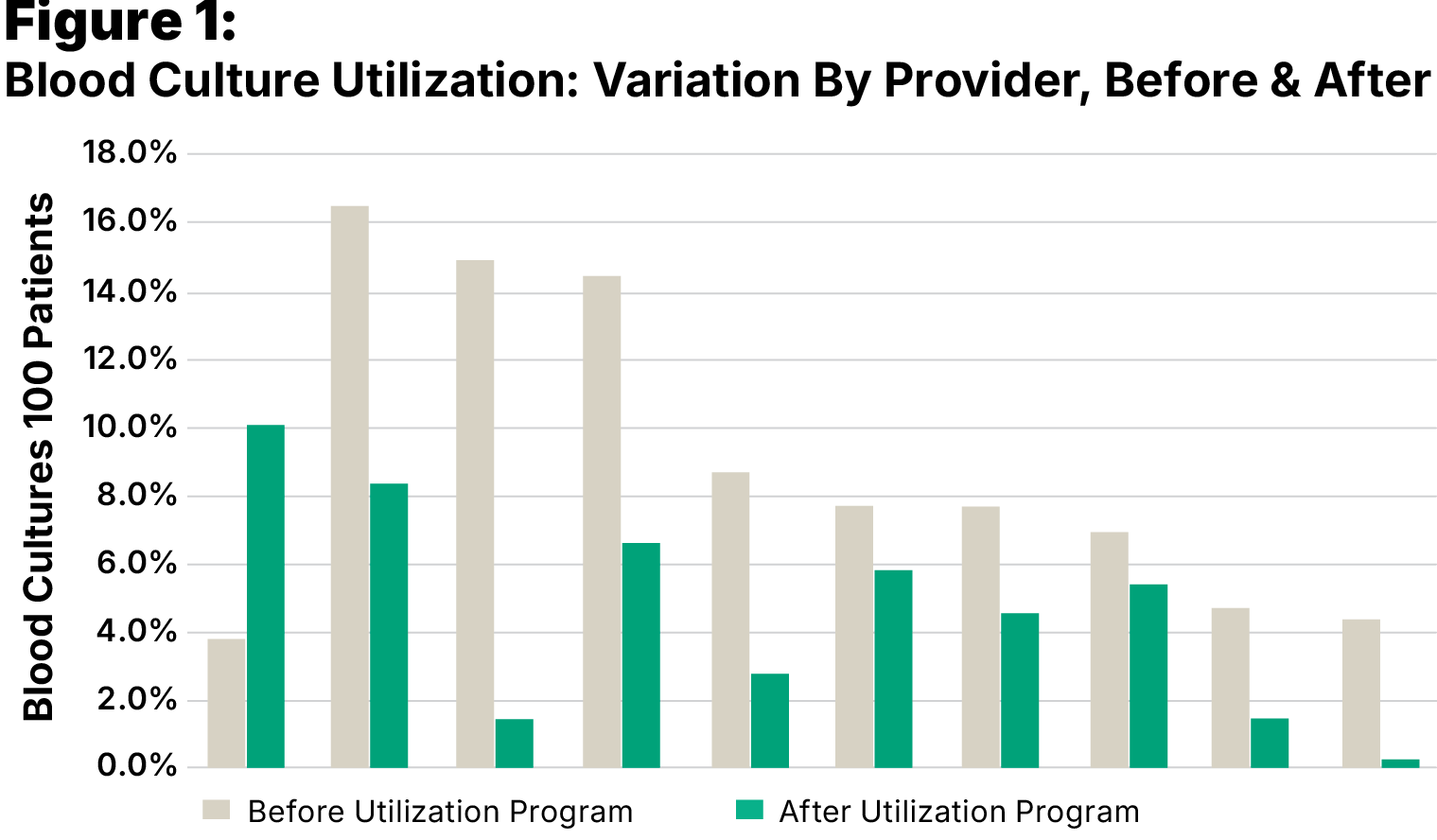
Figure 1: Blood Culture Utilization: Variation By Provider, Before & After
In the beginning, we attempted to simply discover why there was such a wide divergence in utilization amongst its providers. What we found is that different providers, including Nurse Practitioners (NPs) and Physician Assistants (PAs) as well as Physicians, each brought with them different standards from their past jobs and practice areas. In the past, there had not been a focus on a need to change behavior.
We compiled individual utilization statistics for each provider over a 1-year period and disclosed them to everyone: doctors, PAs, and NPs. The reaction was very positive, and it started a constructive conversation about individual standards. Perhaps not surprisingly, few had thought seriously about those standards, or of the consequences of ordering blood cultures when it came to the downstream effects of the testing. Many ER doctors never see their patients again after the initial treatment, which makes them less aware of what happens beyond the ER. Openly discussing these factors helped to bring awareness of the problems associated with unnecessary testing.
The Hawthorne Effect
Almost immediately, blood culture utilization began to drop. We attribute this immediate improvement to the Hawthorne Effect: the mere observance or study of a group of people will change that group’s behavior. In other words, simply by effectively measuring, tracking, and disclosing providers’ usage, we began to reduce utilization.
But we went further, embarking on a comprehensive program designed to educate providers on the downstream costs, be they in increased expenditures or poor patient outcomes. Inservice training on how to properly draw blood cultures began for nursing staff. This training was designed to reduce the rate of blood culture contamination and further reduce downstream costs such as unnecessary hospital admissions, antibiotics treatment, or further testing.
This program not only reduced utilization, it reduced the variability between providers.
| The Results
Savings to the Hospital
At the start of this program, our Physicians ordered blood cultures for 8.76 percent of all patients. After ten months of steady reduction in utilization our Physicians ordered the test at a rate of 4.41 percent (Fig. 2).
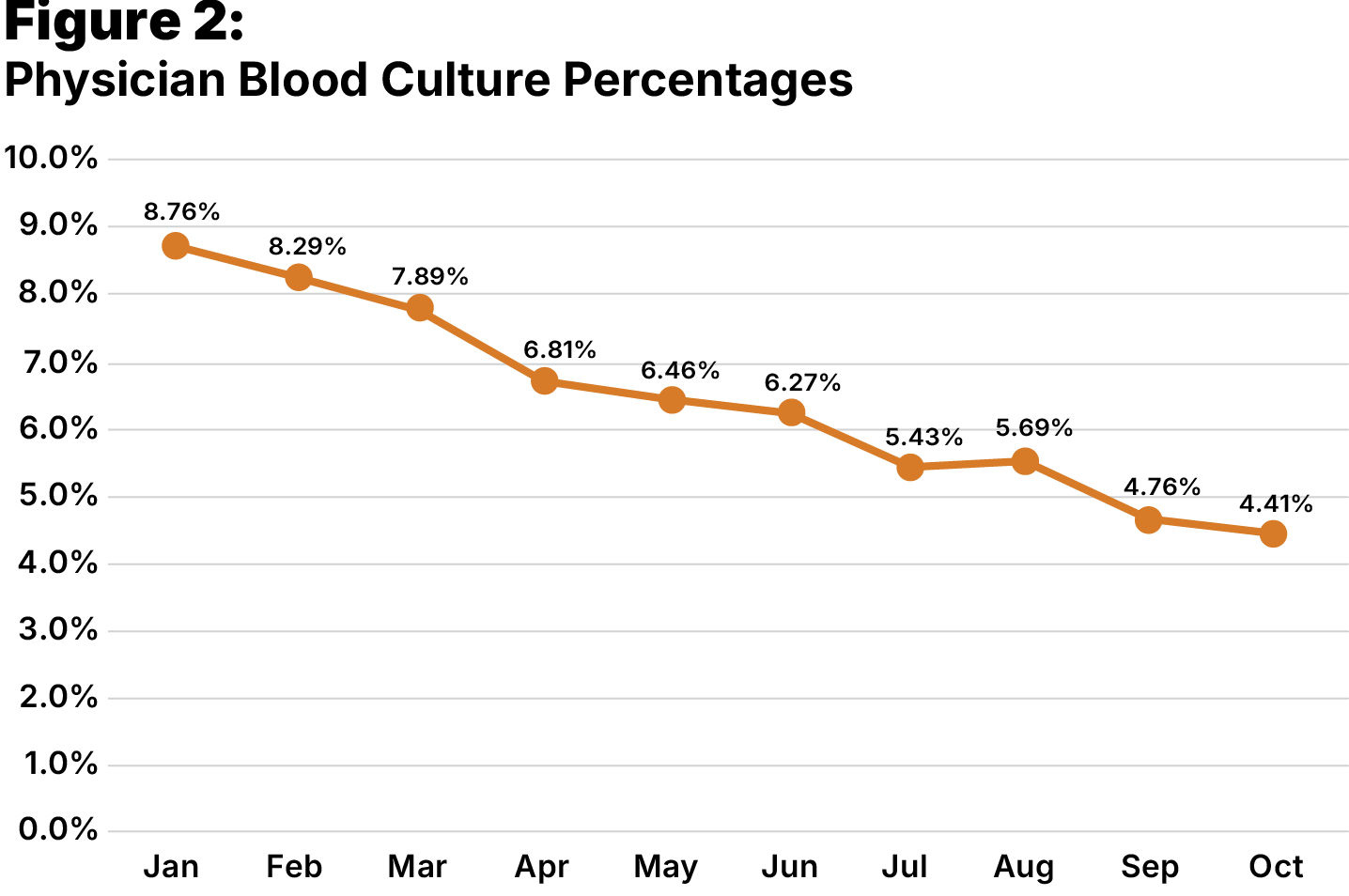
Figure 2: Physician Blood Culture Percentages
The effort to reduce contaminated blood cultures further reduced costs elsewhere. Research shows that each contaminated blood culture leads to $7,000 to $9,000 in downstream medical costs. Altogether, our blood culture program saved our hospital partners a potential $2 million in its first year.
But there are many other opportunities for similar programs. Having seen very real results from their first steps, we expanded our programs to include other testing procedures, including urine, stool, and wound cultures, with mounting success in each area. We are committed to monitoring and evaluating our own performance, and remain focused on improving outcomes, both in terms of patient care and improved financial performance for the hospitals we serve.
New Partnerships
New Opportunities
If you’d like to explore all USACS can offer your facility and join our nationwide network of partners, contact us today.
